Abnormal clotting
- Abnormalities in physiological haemostasis can lead to excessive bleeding
- This can be due to inherited disorders, such as genetic deficiencies in coagulation factors
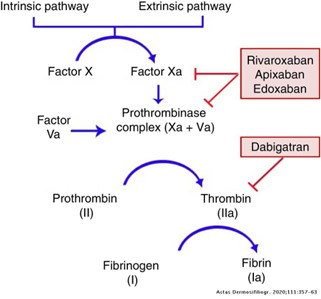
- Medical interventions can also lead to abnormal clotting, such as direct oral anticoagulants (DOACs) that inhibit specific components of the coagulation cascade
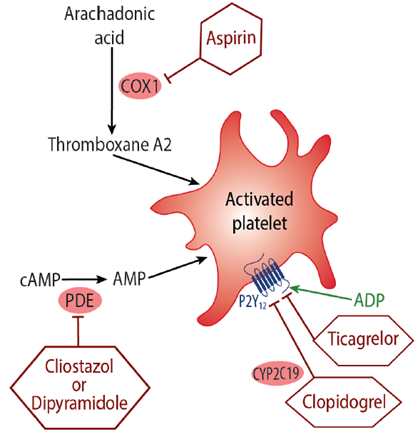
- Anti-platelet drugs, such as clopidogrel, ticagrelor, prasugrel and aspirin, attenuate platelet aggregation and inhibit thrombus formation
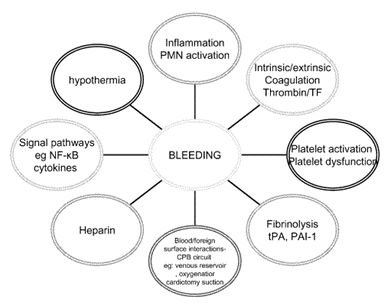
- Surgical interventions, particularly those leading to excessive blood loss, will also have a direct effect on the availability of platelets, fibrinolysis and coagulation factors
Image