Fibrinolysis is difficult to measure directly using conventional laboratory tests.7 Standardised methods to detect abnormalities in fibrinolysis are not as simple or widely available as those used to measure blood clotting.21–23
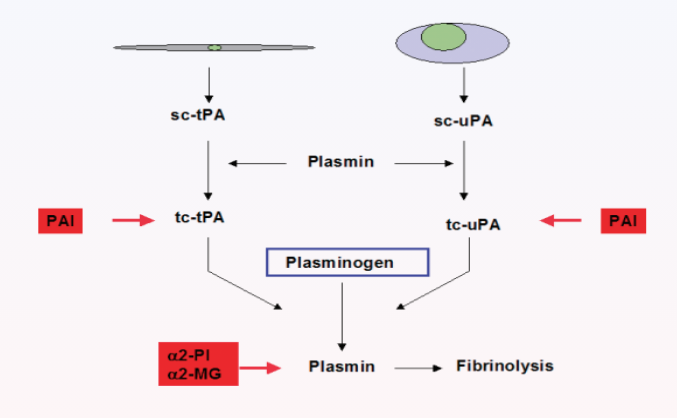
Assessment of euglobulin clot lysis time can be used as a measure of fibrinolysis. Alternatively, antigen tests for plasma proteins involved in fibrinolysis, such as tissue plasminogen activator (tPA), plasminogen activator inhibitor 1 (PAI-1) and thrombin-activatable fibrinolysis inhibitor (TAFI) can be assessed.21–23 Fibrin degradation products, such as D-dimers, are another parameter that can be measured.
D-dimers are late-stage fragments released when fibrin, cross-linked by factor XIII, is degraded by plasmon.9 Circulating D-dimer levels are therefore a measure of fibrin breakdown and ongoing fibrinolysis.9,12 In a clinical setting, D-dimer tests are restricted to the exclusion of thrombosis, due to their low specificity.21,22